- I. Introduction
- II. A Fictional Narrative of a Section 166.046 Dispute
- III. Section 166.046: Historical Background and Black-Letter Law
- IV. The Current Unconstitutionality of Section 166.046’s Committee Review Process
- V. Sun Hudson and Tinslee Lewis: Nonfictional Patients
- VI. Why We Need to Protect Section 166.046: Sun Hudson and Tinslee Lewis
- VII. Suggestions to Correct Insufficiency of Due Process
- VIII. Conclusion
I. Introduction
Since the enactment of TADA in 1999, pediatric medical advancements have taken off.[1] While medical advancements prolong patient lives, sometimes, what is broadcast as a prolongation of life is merely the prevention of biological death.[2] Some argue that prolongation of life and prevention of death are the same and that both align with the constitutionally protected right to life;[3] however, they are not the same. We must distinguish between prolonging life and preventing biological death to reach the root understanding of life as it applies to the constitutional right.[4]
Section 166.046 is a legal tool meant to (1) distinguish between the prolongation of life and prevention of biological death; and (2) prevent the latter for ethical reasons. Specifically, Section 166.046 accomplishes both by allowing physicians to discontinue life-sustaining treatment (LST) when a medical or ethical review committee deems continuation of LST to be “medically inappropriate.”[5]
This Note introduces Section 166.046 through fictional and nonfictional applications to ensure a complete understanding of the black-letter-law analysis also contained within this Note. Additionally, this Note details the current unconstitutionality present in Section 166.046’s procedural guidelines and proposes solutions to correct its constitutional failures. The following definitions (or undefined terms) are critical to understanding this Note:
-
A patient becomes a “[q]ualified patient,” for Section 166.046’s applicability, when their attending physician diagnoses and certifies in writing that the patient has a terminal or irreversible condition.[6] Notably, Section 166.046 applies to both adult and pediatric patients; however, this Note only contains analysis pertaining to pediatric patients.[7] Additionally, this Note’s use of the word “patient” encompasses the term “qualified patient,” as well as the patient themselves and the patient’s parents or legal guardians.
-
The term “‘[a]ttending physician’ means a physician selected by or assigned to a patient who has primary responsibility for a patient’s treatment and care.”[8] This Note’s use of the word “physician” encompasses the definition assigned to “attending physician.”
-
An “advance directive” is a legal instrument executed on behalf of a patient containing instructions to physicians regarding the “administ[ration], withhold[ing], or withdraw[ing] of life-sustaining treatment in the event of terminal or irreversible conditions.”[9]
-
LST is treatment that is “based on reasonable medical judgment,” without which the patient would certainly die. Such treatment includes necessary medications and artificial life support, such as “mechanical breathing machines, kidney dialysis treatment, and artificially administered nutrition and hydration.”[10]
-
“Medically inappropriate” remains undefined.[11]
-
“Committee” remains undefined.[12]
II. A Fictional Narrative of a Section 166.046 Dispute
Before jumping into the non-fictional analysis, this Note provides a start-to-finish theoretical reality of the procedural process, as an attempt to provide a high-level humanization of the black-letter procedural law. Why? Because the application of Section 166.046’s black-letter law to fictional----but realistic----examples is necessary to grasp the gravity of deciding to terminate the LST of a child. Section 166.046 affects real people, and to spark any true change, the legal analysis needs to go deeper than a law review article where the author tries to sound smart.
A. Phase 1: Pre-hospital
A little girl races her bike down the street with friends. The bike streamers flutter through the wind. The little girls laugh. But, out of nowhere, the bike flips; she crashes headfirst into the curb; her skull cracks; and she blacks out with blood pooling underneath her. Thankfully, a neighbor runs out and starts CPR while one of the friends runs to grab the girl’s mom and another calls 911.
B. Phase 2: Emergency Department
The “Red Phone”[13] rings once before the triage nurse grabs it and presses it to her ear. It’s the fire department. A ten-year-old girl, Jane Doe, is being brought into the emergency room. She is ten minutes out.
The little girl arrives at the hospital. EMTs unload her from the ambulance and into the emergency department. A nurse directs other patients out of the way, and the little girl’s stretcher makes it through the crowded halls quickly and easily. She is unloaded from the stretcher, and the emergency department team works silently while EMS gives a report to the head physician.
The patient technician connects the little girl to the monitors; two nurses each insert an IV and draw blood; another nurse preps the antibiotics; a different technician rushes to grab blood for an infusion; and the X-ray technician quickly snaps the necessary images. All the while, the child life specialist stands by the little girl’s head, and even though she is unconscious, she whispers soothing explanations about what’s going on.
Then, the monitor flatlines. If you can look past the fear, the cohesiveness is beautiful. Nobody panics. The nurse draws up the sedative and paralytic; the resident preps for intubation; the respiratory therapist sets up the ventilator; and the head physician monitors everything. In no time, the little girl is intubated and connected to a ventilator, and nurses rush her to the CT scanner.
Thirty minutes later, the hospital social worker and child life specialist usher the girl’s parents into the room. They see their little girl. There are tubes and wires everywhere. They look to the nurse and start asking questions, but they only speak Spanish, so the nurse calls the translator. Once the translator arrives, the physician asks the parents for the girl’s name. The physician goes on to explain everything they’ve done so far, but the sound of the monitor flatlining again interrupts the physician. After six rounds of advanced-care life support, their daughter’s pulse returns.
The attending physician walks out of the room. She’s sweating. Despite her twenty-six years of experience, her hands still tremble every time the monitor flatlines. She sits down at her computer and sees that the CT and blood results are in. It’s bad. She picks up the phone and calls the ICU attending. She goes over the medical history, the reason for admission, the treatments undergone, and the diagnostic results. “Code status?” “Full code.”
C. Phase 3: Admission to the ICU
Before the little girl is transferred to the ICU, she flatlines once more. Once there, the stress of the transfer causes her to flatline again. For the rest of the night, that same flatline noise can be heard from the monitor repeatedly.
It’s nine weeks after the little girl’s accident. For the millionth time, the physician looks at the imaging, the labs, and the procedures already performed, but she can clearly see that this little girl is not coming back. The physician stands up and heads to the girl’s room with the translator. Her parents are there—just like they have been every day for the past nine weeks. The girl is thinner than she was, there are more tubes than before, and her vitals are still unstable. The physician asks the parents to sit down and explains to the family, again, that all these treatments are just being done to the little girl rather than for her. Her mom starts to cry silently, but the physician continues. She explains that, at this point, withdrawal of LST would be the most humane thing to do; moreover, continuing to stick her with needles, shock her chest, and stick tubes into her would be cruel and futile.
All the parents can hear is that the physician wants to stop trying to keep their child alive. They look over at their child. They see her laying in the bed next to this conversation. IV pumps are beeping. The monitor shows that she has a heart rate and her chest is rising and falling. Her parents have been sitting next to her bed, holding her hand, and begging for her life. They refuse to give up on their child. It’s a miracle that she is still alive, which, to the parents, means that their child—their strong little girl—is meant to make it through this; so, like before, the girl’s parents refuse to give up on her. They tell the physician that they refuse to discontinue LST.
D. Phase 4: Starting the Section 166.046 Process
The physician walks out of the room and takes a deep breath before she heads to the director of the hospital ethics committee. Once in the director’s office, the physician explains that she refuses to abide by the parent’s decision to continue providing LST, and she wishes to begin the Texas Advance Directives Act’s § 166.046 process.
E. Phase 5: 48 Hours Before the Committee Convenes
Forty-eight hours before the committee convenes, the hospital sends a representative to the child’s room. The representative hesitantly knocks on the door before walking into the room. The representative makes an introduction to the child’s parents and tells them what is going on.
While the machines beep all around them, the representative hands the parents a written description of the ethics or medical committee review process along with the healthcare facility’s policies and procedures specific to TADA. The representative takes a deep breath and informs the parents that, in forty-eight hours, an ethics or medical committee will convene to decide whether continuing their child’s LST is medically inappropriate.
The parents are informed that if the committee agrees with the doctor, LST will be withdrawn after ten days if no transfer of care can be arranged. The child’s parents are startled at the time constraints and the process. The representative has no good answer to ease the parent’s concerns about the forty-eight-hour turnaround; however, the representative does assure the parents that the girl’s doctor will not be part of the ethics or medical committee and that all LST will be continued throughout the review process.
All signs point to fighting an uphill battle. Fear hits the parents, and the need for more information takes the forefront of all thought. The representative informs them that they are entitled to attend the meeting. Then, the representative informs them that, on top of hearing the decision first-hand, they will also receive a written explanation of the committee’s decision, a copy of their child’s medical records, and a copy of her diagnostic results and reports. Before leaving, the representative hands the parents a list of healthcare providers and referral groups that might be able to aid with the transfer of their child if the committee decides against them.
The parents are left with a bunch of papers in their hands and even more questions. Is there a Spanish version of these documents? What does “medically inappropriate” mean? Will there be a translator there to help them plead their case? They aren’t doctors, so who will tell the committee why their daughter’s doctor is wrong? What evidence does the committee usually rely on? How much proof does the committee need? How often does this process occur? How can they prove to the committee that their daughter’s life-sustaining treatment should be continued? Are nonmedical factors considered? Are their religious beliefs considered? Do they have a say in who is on the committee? But nowhere in the documents are the answers to those questions.
F. Phase 6: Section 166.046 Review Committee
The child’s parents walk into a room full of people that they don’t know—a room full of people that don’t know their child. Nevertheless, a room full of people who will decide whether their child lives. The parents take their seats, and the meeting begins. The doctor stands up and starts talking about their child’s medical history. Medical words are thrown around, and the prognosis is discussed. After that, the doctor tells the room that it would be medically inappropriate to continue LST. Then, the parents stand up and beg the committee to decide the contrary—to decide that their child deserves the LST that will keep her heart beating. The parents don’t have years of medical training or experience to combat the doctor’s medical conclusions. All they have is the ability to plead for their child’s life.
While the committee debates, the parents take their spots next to their child’s bed. They hold her hand. They pray. They cry. They watch the monitor to make sure her heart is still beating. Finally, the representative knocks on the door again. The committee decided that the doctor is right—it is medically inappropriate to continue the child’s LST.
G. Phase 7: Seeking Transfer
The clock starts ticking. The parents have ten days to find a new healthcare facility that will accept their child as a transfer patient. Every possible second of those ten days is spent trying to locate a safe haven for their child. The parents call every number on the registry. They send the copies of the medical records and diagnostic results provided to them. They coordinate calls between the other facilities and the current one.
H. Phase 8: Discontinuing LST
But the tenth day comes and goes, and no other healthcare facility has accepted the child’s transfer of care. The doctor, nurses, healthcare-facility representative, child life specialist, and chaplain walk into her room. Her parents grasp her hands while the doctor discontinues all LST. Eventually, her heart no longer beats, and her chest no longer rises: their child is gone.
The nurses and the child life specialist move about the room quietly, trying to give these grieving parents as much privacy as possible. The child life specialist creates fingerprint keepsakes and tucks a stuffed animal into the crook of the child’s arm. The nurses put a warm blanket over her, but they stop before they cover her face. “Do you want a moment alone?” The parents are left alone with her. No more beeping monitors. No more rise and fall of the chest. The nurses come back in and cover the child’s face. They watch as her body is placed into a body bag, and the pain swallows them whole.
The doctor sits at home that night—silent. She runs through every decision they made for that child: all the tests they ran; the procedures they performed; the things that were being done to her instead of for her; the pain inflicted through needles, procedures, tests, and tubes—pain that only served to prolong the inevitable: death. In her mind, the doctor replays the sobs of parents over and over and over again. She sees the child’s face every time she closes her eyes. “It was the right thing to do. She’s not suffering anymore.”
III. Section 166.046: Historical Background and Black-Letter Law
What the fictional narrative above illustrates is Section 166.046’s “legally sanctioned extrajudicial process for resolving disputes about end-of-life decisions.”[14] The disputes Section 166.046 intends to resolve are between physicians and the patient; specifically, it is intended to resolve when a physician refuses to continue LST and that refusal directly contradicts the patient’s advance directive or treatment decision.[15] At the crux of the dispute is the term “medically inappropriate”—an undefined and historically disputed term.[16]
A. Section 166.046’s Enactment Background
The Texas legislature enacted Section 166.046 in 1999. The critical issue within a qualifying dispute is whether withdrawal of LST would be “medically inappropriate;” but, “medically inappropriate” stems from medical “futility”—a highly debated issue in both the medical and legal communities before this section’s enactment.[17]
In the 1970s, medicine advanced to a point where medical, ethical, and legal principles were forced to collide, and the question of medical “futility” became a prominent issue in both the medical and legal communities.[18]
In 1976, the collision of medical, ethical, and legal principles reached the New Jersey Supreme Court through the case In re Quinlan.[19] In re Quinlan was the first judicial recognition that terminally ill patients have a constitutionally protected liberty interest to voluntarily refuse life-sustaining treatment.[20]
Alternately to the Quinlan court, physicians have argued that when medical interventions fail to serve a “therapeutic or palliative purpose,” they are “medically unnecessary and inappropriate,” and thus, “futile.”[21] Further, when deemed futile, withdrawal of LST is both ethically and medically obligated.[22] For support, physicians cited the Hippocratic Oath and the goals of medicine generally:[23] (1) the primary rule of the Hippocratic oath is “first, do no harm;”[24] and (2) the three goals of medicine are cure, relieve suffering, and refuse treatment to “those ‘overmastered by their illness.’”[25] In short, physicians argued that continuing medical interventions with medically futile patients is an unethical, impermissible violation of physicians’ oaths and medicine as a whole.[26]
Despite the physicians’ arguments, the courts often sided with families’ decisions regarding the futility of treatment.[27] As a result, physicians made efforts to define “medical futility” themselves.[28] In the quest to define “medical futility,” debate amongst scholars erupted.[29] Disagreements between who should be defining futility and what futility even means were at the center of the debates.[30] As to who should be defining futility, scholars were split between physicians and healthcare institutions.[31] Proponents of physicians argued that the physicians should “distinguish between everything that can be done and everything that should be done,” whilst healthcare institutions should only develop guidelines.[32] As to the what, scholars were split between “physiologic, quantitative, and qualitative” definitions of futility.[33] Throughout these debates, some healthcare institutions and general communities developed varying policies for defining and handling medical futility.[34]
In 1999, the American Medical Association (AMA) Council on Ethical and Judicial Affairs released guidelines for interpreting medical futility that addressed the institutional questions but left unanswered the pending legal question of exactly what medical futility is.[35] The guidelines provided a process-based approach for defining medical futility rather than a standard definition.[36] The process-based approach mimicked the methods applied by major ethics committees: counseling and deliberation between the opposing parties.[37] A lack of agreement would result in an attempt to transfer care to another facility.[38] Per the AMA council, “if no resolution was . . . [reached] and no transfer [of care] to a willing provider could be arranged,” then it was ethically permissible to terminate medically futile interventions.[39]
Because the question of legality remained unresolved, a Texas multidisciplinary task force composed of lawmakers, lawyers, physicians, pro-life groups, and other stakeholder groups came together to “set[ ] forth uniform provisions governing the execution of an advance directive” regarding health care.[40] The result was the consolidation of three pre-existing laws into one single law—§ 166.046 of the TADA.[41]
Like the AMA council, the drafters of the statute failed to provide a definition of medical futility.[42] The drafters conceded that there would never be a standard definition for futility that would satisfy the wide array of situations this law could potentially affect.[43] Thus, the word “futility” was left out of the statute.[44] Instead, TADA focused on the creation of a “legally sanctioned extrajudicial process for resolving disputes about end-of-life decisions.”[45] Thus, the who that would resolve these disputes would be a medical or ethical committee that the physician at issue could not be a part of, and what this committee would decide was whether continuation of LST would be medically inappropriate.[46]
B. Section 166.046’s Black-Letter Law
Section 166.046 creates an extrajudicial process that culminates in a singular determination by an “ethics or medical” review committee: whether the continuation of LST would be “medically inappropriate.”[47]
As the statute stands, the patient must be informed of the committee review process, in writing, at least forty-eight hours before the committee meeting.[48] Additionally, at the meeting, the patient or their legal representative must be provided a copy of the Section 166.052 statement and a list of entities willing to aid in the transfer of care.[49] These entities consist of healthcare providers and referral groups willing to either consider an acceptance of transfer or assist in locating a willing transfer provider.[50] Under the statute, a patient or legal representative has the uncontested right to (a) “attend the meeting;” (b) “receive a written explanation of the decision;” (c) “receive a copy of the . . . patient’s medical record” that discloses the relevant treatment; and (d) “receive a copy of all . . . diagnostic results and reports” pertaining to (c).[51]
At the committee meeting, a decision is reached as to whether the physician has correctly deemed that continuation of LST would be medically inappropriate.[52] While Chapter 166 of the Code contains an entire section dedicated to defining the terms within, a definition of “medically inappropriate” is not provided.[53] Thus, medical inappropriateness—the essential verdict to be decided by the committee—is left to the conceptualizations of the committee.[54]
If the committee’s final—and given the lack of guidance, wholly subjective—determination is that it would be “medically inappropriate” to continue LST, withdrawal of LST is permissible and protected by law; however, this determination does not result in immediate discontinuation of LST.[55] First, the physician and healthcare institution must continue to provide LST for ten days after the committee’s written decision is provided to the patient’s parents or guardian.[56] Second, the physician and healthcare institution must make reasonable efforts to aid in the transfer of the patient to another physician, care setting, or facility.[57]
Ten days after the committee’s decision, legal protection is triggered, and the physician and the healthcare institution are no longer obligated to continue providing LST to the child.[58] However, an extension past the ten-day period may be granted if the court finds that there is a reasonable expectation that an alternate physician or healthcare facility will accept the transfer of care.[59] If the court finds that a reasonable expectation exists, the attending physician and healthcare facility must continue LST until the extension expires.[60] Then, withdrawal of LST is permissible and protected.[61]
IV. The Current Unconstitutionality of Section 166.046’s Committee Review Process
Section 166.046’s current procedural guidelines fail to meet the “elementary and fundamental requirement of due process in any proceeding”—sufficient notice for all parties to have the “meaningful opportunity to be heard” and object based on “the practicalities and peculiarities” of the circumstances.[62]
A. Section 166.046: Unreasonable & Meaningless
Currently, a physician is not required to notify the patient about a review process until forty-eight hours before the review committee convenes.[63] This current notice window violates due process requirements because it does not “afford a reasonable [notice] time,” which further prevents a “meaningful opportunity to be heard.”[64]
For patients to have both reasonable notice and a “meaningful opportunity to be heard,” they must be able to adequately prepare to advocate and have time to advocate in support of their interests with an understanding of the level of advocacy required.[65]
A due process analysis for reasonableness of time requires consideration of (1) the interested parties; and (2) the circumstances.[66] Here, the interested parties include the physician refusing to continue LST and the patient. The circumstances involve patients whose medical conditions are critical enough to warrant LST; thus, the nature of the decision to withdraw LST based on medical inappropriateness calls for “reasonable medical judgment” involving highly complex diagnostic and prognostic considerations based on objective medical evidence and considerations.[67] Thus, the review committee’s determination turns on medical evidence; however, while both parties are privy to the circumstances, the equal playing field stops at lay-witness evidence, because only one party is a physician.
In a dispute involving reasonable medical judgment, both parties must be provided sufficient notice “to obtain and present witnesses and documentary evidence” that supports their position and may be used to rebut the other side’s position.[68] When combining this with the fact that the patient representative is often not a medical expert in the relevant medical field,[69] the only way to rebut a physician’s position is by obtaining a medical expert. If the patient representative shows up to the review committee meeting without their own medical expert due to insufficient notice, they will not have a “meaningful opportunity to be heard,” and the decision reached will be without the support of “constitutional adequacy.”[70]
Accordingly, notice is constitutionally adequate only if it allows reasonable time to retain an expert for a “second opinion.”[71] Calling back the complex nature of Section 166.046 determinations, “second opinion” experts must have reasonable opportunity—and thus, reasonable time—to fully analyze the objective medical data so that they may “refute . . . [the patient’s] terminal or irreversible condition diagnosis, confirm continued life-sustaining treatment as medically appropriate, or otherwise demonstrate a more optimistic survival prognosis.”[72]
A patient is not being afforded the notice necessary to advocate because Section 166.046 does not provide all interested parties sufficient time to present evidence, secure expert medical testimony, or cross-examine witnesses testifying in support of the discontinuation of LST; and it is thus, constitutionally insufficient.[73]
B. Section 166.046 Committee Review Process: Blind and Mindless Decision Maker
The entity making the final determination is an “ethics or medical committee.” While, technically, this review committee is the decision maker in the dispute, Section 166.046’s current unconstitutional failures essentially make the attending physician the only party able to advocate for a decision in a manner considered sufficient to satisfy due process requirements.[74] Accordingly, the attending physician is the only side truly able to influence the committee—essentially making the committee the physician’s agent.
This section explores the committee review process in its current unconstitutional state.
1. “Defining” a Section 166.046 Committee
Beyond the fact that the committee must be an ethics or medical one, Section 166.046 is silent on what a committee is made up of; however, § 166.002 of TADA provides slightly more insight. Under Section 166.002, an “‘[e]thics or medical committee’ means a committee established under Sections 161.031–161.033.”[75] At the behest of Section 166.002, we look outside of the Advance Directives chapter to Chapter 161: Public Health Provisions, in search of insight into a Section 166.046 “ethics or medical committee.”
Section 161.031 of the Code adds some meat to the meaning of “medical committee” as used in Section 166.046:
MEDICAL COMMITTEE DEFINED. (a) In this subchapter, “medical committee” includes any committee, including a joint committee, of:
(1) a hospital;
(2) a medical organization;
(3) a university medical school or health science center;
(4) a health maintenance organization . . . ;
(5) an extended care facility;
(6) a hospital district; or
(7) a hospital authority. [76]
While finally providing the most direct definition yet, it still fails to provide a clear understanding of what a Section 166.046 medical committee entails.
As to “ethics committee,” the sections only offer more silence by failing to provide even a vague definition associated with the term. In fact, Chapter 161 is generally silent as to the evaluation of ethical dilemmas. In following the current terms of the Code, we must consider the failure to define “ethics committee” as intentional and, thus, assign the provided definition for “medical committee” to “ethics committee” as well.
By (1) assigning the definition for “medical committee” to “ethical committee;” and (2) failing to outline the “who” of the committee, another issue arises—an issue of intended purpose. According to Section 166.046, the committee’s purpose (whether a medical or ethical committee) is to resolve disputes about end-of-life decisions; however, Section 161.0315, a section we are guided to by Chapter 166, limits the committee’s scope of evaluation to medical and healthcare services only.[77] While a committee determination certainly requires the evaluation of medical and healthcare services, the scope of evaluation should also encompass ethical, religious, and cultural considerations—amongst other things.
2. The “Who” of the Committee
After “defining” a Section 166.046 committee, the referenced Chapter 161 sections go on to note that the Code empowers the governing bodies of the above seven entities with the ability to create a committee and select its members.[78] Beyond that, the Code provides no guidance or limitations as to the “who” of the committee beyond the fact that the attending physician cannot be a committee member.[79] Because Section 166.046 does not require public reporting of committee composition, finding out the “who” of a committee is difficult; however, judicial opinions offer some insight.[80]
Recently in T.L. v. Cook Children’s Medical Center, the Fort Worth Court of Appeals issued an opinion that broke down the composition of the committee involved with that specific patient.[81] Tinslee Lewis’s review committee was initially a twenty-five-person committee; however, of the twenty-five total committee members, only twenty-two showed up.[82] Nineteen of whom were active Cook Children Medical Center’s employees, and the remaining three were nonmedical members.[83]
3. No Protection from Bias and No Representation in the Committee
The information available as to the Tinslee Lewis committee calls attention to issues of representation present due to the failure to include any guidelines pertaining to committee-member qualification. As it currently stands, it seems that committee members will only be a “jury of peers” for a physician but never for a non-white patient, thus implicating severe bias.[84]
Section 166.046 contains no procedural guardrails to enforce the Fourteenth Amendment’s mandate that an impartial adjudicator of disputes make the determination when the right to a protected interest—like the right to life—is at stake.[85] The potential for bias in determining “medical inappropriateness” is painfully obvious considering that the attending physician’s colleagues often make up the review committee.[86] This is not a fair and impartial forum.[87] Without “[a] fair trial in a fair tribunal,” due process has not been satisfied.[88]
Further, there is no requirement that “statutory duties exist with respect to the identity, skills, or training of the committee members” who make up the review committee.[89] How can a review committee consisting solely of lay people make a decision based on “reasonable medical judgment”? It cannot. Without the requisite skills to understand the provided evidence—one-sided as it might currently be—the review committee merely acts as a “check on [potentially] less-than-altruistic medical coercion.”[90]
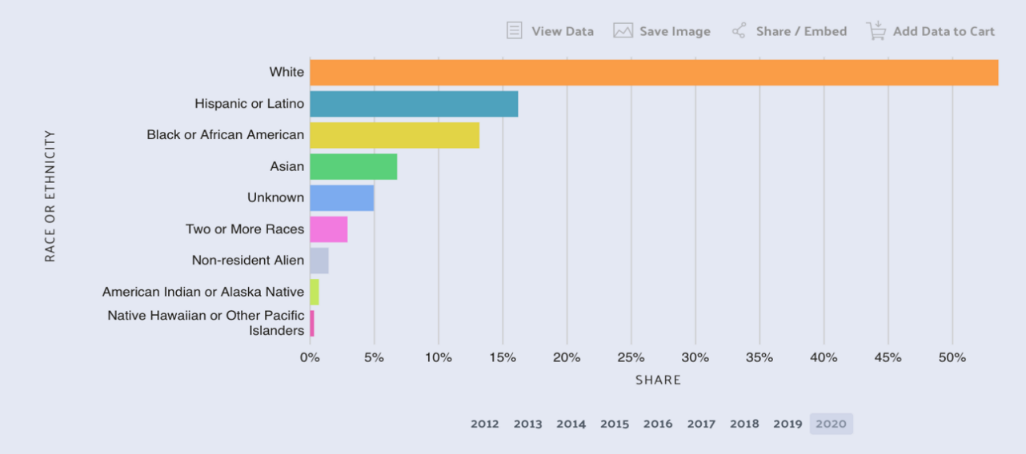
Finally, a 2020 collection of data revealed that 53.6% of degrees awarded in healthcare went to white students, 16.2% went to Hispanics or Latinos, and 13.2% went to Blacks or African-Americans.[91]

With numbers like this, non-white patients will likely never have a dispute reviewed by a jury of their peers.
4. Subjective Mystery of the Committee’s Determination
Even ignoring the aforementioned arguments, a patient still does not have the requisite “meaningful opportunity to be heard” because the crux of the review committee’s determination is not only wholly subjective but also a subjective mystery.[92]
The term “medically inappropriate” controls the binding, life-or-death determination made by the review committee.[93] Yet, there is no provision for what “medically inappropriate” means. In fact, nothing within the entirety of Chapter 166 provides an objective understanding of what the term means.[94] Furthermore, no reference to other terms, other legislation,[95] or other objective factors is included to guide the review committee or the interested parties in interpreting the term “medically inappropriate.”[96]
Current procedural standards are ad hoc and thus, leave a patient blind as to the evidence necessary to advocate in support of their interests.[97] What’s more, to abide by the reasonable medical judgment, the lack of ascertainable definitions or guidelines essentially substitutes an objective evidentiary standard with the physician’s ipse dixit.[98] Therefore, patients’ ability to advocate for their position is substantially limited, resulting in no meaningful opportunity to be heard.[99]
V. Sun Hudson and Tinslee Lewis: Nonfictional Patients
Sun Hudson was the first pediatric patient to which TADA § 166.046 was applied,[100] and Tinslee Lewis is a recent pediatric patient under the same spotlight.[101] Sun and Tinslee’s physicians both called upon Section 166.046 to discontinue LST on pediatric patients born with fatal congenital diseases,[102] and both situations resulted in legal processes that went beyond Section 166.046’s procedural framework.[103] This part details the medical and legal issues particular to each patient.
A. Section 166.046’s First Pediatric Patient: Sun Hudson
Sun was born in September 2004 at St. Luke’s Hospital in Houston, Texas.[104] At birth, Sun suffered significant respiratory distress that required intubation, placement on a ventilator, and a transfer to Houston’s Texas Children’s Hospital.[105] After genetic testing, it was discovered that Sun was born with thantophoric dysplasis, which is a rare, typically fatal form of congenital dwarfism.[106] Because of this disease, he was born with an abnormally narrow chest cavity that restricted his ability to breathe—to the point of suffocation.[107] Most babies born with this disorder die within a few days of birth due to the respiratory restrictions, but Sun survived nearly six months.[108] Essentially from birth until death, he was suffocating, but just not enough to die due to the medical care available at Texas Children’s Hospital.[109]
Sun lived in this state of restricted respiratory capacity because his mother, Wanda, refused to discontinue LST despite physician recommendations to do so.[110] Sun’s physicians explained to Wanda that his condition had no medical treatment, and that he was in pain any time he was not fully anesthetized.[111] Still, Wanda refused to discontinue LST.[112] Her refusal was based on her delusion that she was impregnated by the sun—hence the name Sun.[113] Wanda wholeheartedly believed that her child was “the sun that shines down in the sky (who) has come down in the flesh and blood.”[114]
After Harris County’s Children’s Protective Services failed to intervene, Sun’s physicians advocated for a discontinuation of LST under Section 166.046.[115] They argued that “[such] care was futile and medically inappropriate.”[116] The review committee agreed.[117] Although not required to, the hospital secured independent legal counsel for Sun’s mother due to her mental state.[118] Wanda, on behalf of Sun, took the matter to court and asked for a temporary restraining order to prevent the discontinuation of LST.[119] Litigation ensued, until finally, on March 14, 2005, a judge allowed the hospital to withdraw LST.[120] The next day, Sun’s breathing tube was removed, and he died within one minute.[121]
B. Section 166.046’s Recent Spotlight: Tinslee Lewis
Since birth, Tinslee was hospitalized at Fort Worth’s Cook Children’s Medical Center in one of its cardiac intensive care units (CICU).[122] She was born eight-weeks premature in February 2019 with a severe form of Ebstein’s Anomaly,[123] a rare, congenital cardiac condition.[124] Where normally a newborn’s heart would occupy forty-to-fifty percent of the chest cavity, Tinslee’s took up ninety percent.[125] In addition to her Ebstein’s Anomaly, Tinslee was also diagnosed with chronic lung disease and severe pulmonary hypertension, which worsened her condition.[126]
1. Triggering Section 166.046
Despite “multiple major” cardiac surgeries, Tinslee had reached a point where she could experience two to three “‘dying’ events” per day, triggered by routine things such as baths and diaper changes.[127] In July 2019, she suffered her worst dying event up to that point; she suffered a severe pulmonary hypertension crisis where none of the usual treatments—sedatives, paralytics, nitric oxide, or intubation—relieved the crisis.[128] Eventually, after emergency surgery, her lungs relaxed sufficiently to go back on ventilation.[129] Unlike before, however, Tinslee was not able to breathe without a ventilator; she now required continuous ventilation and constant sedation.[130] The constant sedation prevented any interaction between Tinslee and her mother, but it was medically necessary to prevent another crisis and accidental self-removal of the lines and tubes connecting her to the medical treatments keeping her alive.[131]
After the July 2019 dying event, Tinslee’s attending physician concluded that continuation of LST would be medically inappropriate.[132] Prior to this conclusion, the attending physician consulted other CICU physicians and her cardiothoracic surgeons.[133] According to the physicians, Tinslee had reached a point where no surgical interventions or medical treatments would lead to eventual improvement; instead, she would require repeated emergent surgical interventions like the one in July 2019.[134] Further, they concluded that she was suffering and any continuation of LST would be “‘cruel’ and ‘unnatural.’”[135]
2. The Actual Carrying Out of Section 166.046
The physicians and nurses began conversations with Tinslee’s mother (Mother) about the medical reality of her condition.[136] Physicians urged discontinuation of LST to allow a natural death.[137] Mother resisted the initial urgings, and eventually refused to even make contact with the physicians.[138] She clung to her religious views and the hope that something could still be done for her daughter.[139] When physicians and nursing staff explained that Tinslee was suffering, she disagreed.[140]
Months of resistance passed, and Tinslee continued to have severe pulmonary hypertension crises despite the constant sedatives and pain medications.[141] After it became clear that there were unresolvable differences in opinion with Mother, her attending physician initiated the TADA § 166.046 procedure.[142]
On September 27, 2019, Tinslee’s physician contacted the Cook Children’s ethics committee chair for a consultation.[143] The chair of the ethics committee first met with the attending physician to confirm the requested consultation.[144] After confirmation, another ethics committee member met with Mother.[145] At this initial meeting, the ethics committee member ensured there was no miscommunication between Mother and the attending physician about Tinslee’s condition and prognosis and explained the ethics committee review process.[146] Not once during this initial meeting was the possibility of the withdrawal of LST discussed.[147] Then, a second discussion took place between the ethics committee chair and Mother.[148] At this second discussion, Tinslee’s medical condition, medical challenges, and methods by which the hospital could help Mother’s hopes for Tinslee were discussed.[149] Again, no discussion of the withdrawal of LST as recommended by the physician took place.[150]
3. Committee Review for Tinslee
“On Friday, October 25, 2019, the [ethics] committee chair notified [M]other,” through a written letter that the ethics committee review would take place on October 30, 2019.[151] This letter was the first form of communication through which Mother was notified that the committee, under TADA, would consider whether the continuation of LST was medically inappropriate.[152] In addition to the letter, the ethics committee chair spoke with Mother personally that day and explained the procedure of the review process.[153]
The ethics committee review meeting took place at noon on October 30, 2019.[154] Those in attendance included Mother and Tinslee’s maternal grandparents, the attending physician, and the actual committee.[155] The twenty-five-person committee included physicians and other health care providers not involved in Tinslee’s care, nonmedical members, and the parent of a former Cook Children’s patient.[156]
The meeting lasted two hours.[157] During that time, the attending physician, Mother, and Tinslee’s grandfather all spoke.[158] The physician recounted Tinslee’s medical history and provided a consensus view of her medical prognosis, and the family members urged the continuation of LST.[159] Before deliberating, the ethics review committee excused the attending physician, Mother, and Tinslee’s grandparents.[160]
“After thirty to forty-five minutes of deliberation[ ], the [ethics review] committee” concluded unanimously that it would be medically inappropriate to continue LST.[161] The committee had no particular evidentiary standards for its decisions; rather, it merely “weigh[ed]” what the attending physician, family, and other speakers had to say at the review meeting.[162] Further, the committee failed to return to an open meeting to announce its decision and failed to formally transcribe both presentations and its deliberations."[163]
The next evening, the committee chair had the nurse supervisor deliver “the statutorily required written notice of the committee’s decision.”[164] The nurse supervisor informed Mother that continued LST would be guaranteed until November 10, 2019.[165] Because of the delivery time of the letter, she had only six business days to possibly obtain a transfer for her daughter.[166]
Throughout those days, the CICU physicians contacted over twenty hospitals—none of which would accept Tinslee as a patient.[167] The attending physician provided an objective medical history and current medical status but did not provide his own prognosis to the possible transfer providers.[168] Based on the conversations, the attending physician did not believe an acceptance of transfer was likely.[169]
4. Tinslee’s Lawsuit
Mother filed a request for a temporary restraining order (TRO) which was approved by the District Court of Tarrant County on November 10, 2019—the same day that the TADA ten-day window would have closed.[170] Along with the TRO, she filed a suit under 42 U.S.C.A. § 1983 and Texas’s Uniform Declaratory Judgments Act.[171]
At the trial court hearing, Mother alleged that TADA § 166.046 deprives patients of constitutionally required due process of law for two fundamental rights: the right to life “and the right to determine the course of medical care.”[172]
Mother argued that she had a probable right to relief based on TADA’s due process failures and its overly vague “best interests” standards of proof.[173] Specifically, she argued that the forty-eight-hour requirement under TADA was not adequate notice, and the mere attendance of a medical review committee, composed primarily of hospital employees, failed as a meaningful opportunity to be heard before a neutral arbiter; thus, due process failed.[174] In addition, she argued that the attending physician and committee member’s personal judgments violated due process because there was no use of “ascertainable standards for determin[ation]” of the final decision—“whether continuation of LST would be ‘medically inappropriate.’”[175] “[T]he trial court denied Mother’s request for a temporary injunction.”[176] She appealed the ruling.[177]
On appeal, a Texas appellate court found that Mother had shown that she had probable right to recover under a viable claim—the § 1983 claim—and that she had established that failure to grant a temporary injunction would result in immediate, irreparable harm—the death of her daughter, Tinslee.[178] The appellate court acknowledged that, “as applied in this instance,” Mother’s pleading that the committee review process under TADA failed to comply with procedural due process was a viable cause of action.[179] According to the court, due process was not satisfied because she did not receive reasonable notice, had no meaningful opportunity to be heard, and Section 166.046 failed to provide an objective evidentiary standard or burden of proof that would meet the constitutional “best interests” standard for terminally ill children.[180]
On July 24, 2020, the appellate court reversed the trial court’s denial of Mother’s request for a temporary injunction and remanded the case to the trial court.[181] Since then, Cook Children’s Medical Center petitioned for a review, but certiorari was denied by the Supreme Court.[182] Currently, the case is still pending to be decided on the merits by the Tarrant County District Court.[183]
VI. Why We Need to Protect Section 166.046: Sun Hudson and Tinslee Lewis
Both Sun and Tinslee’s parents’ opposition to withdrawal of LST resulted in their children’s suffering—suffering that, while this Author wholeheartedly believes was unintended and undesired by the parents, was inflicted, nonetheless.
The decision by Sun’s mother to ignore physician recommendations for discontinuation of LST led to six months of near suffocation for him.[184] Sun’s doctors explained to his mother that he was in pain and that his condition was irreversible, but still, their appeals fell on deaf ears.[185]
The decision by Mother to ignore physician recommendations for discontinuation of LST led to a 2.5-year legal battle under TADA.[186] During that time, physicians explained to Tinslee’s mother that her condition was irreversible and that she was suffering.[187] Just like with Sun’s physicians, the opinion of Tinslee’s physicians has remained unchanged: “There remains no hope for recovery.”[188] However, her physicians went a step further by arguing that continuation of treatment would result in a violation of their physician oath: “primum non nocere (‘first, do no harm’).”[189]
In both examples, physicians advocated for discontinuation of LST because the patient had reached an irreversible point in their health where continued treatment would only cause suffering.[190] That is exactly TADA’s intended purpose—legal discontinuation of LST when such treatment would be medically inappropriate. However, as time has progressed since the enactment of Section 166.046, TADA’s achievement of its intended purpose has been barred by procedural unconstitutionality. To rectify its current ineffectiveness, constitutional corrections to the procedural guidelines must be implemented to achieve due process sufficiency under the Fourteenth Amendment.
VII. Suggestions to Correct Insufficiency of Due Process
Due process protects people from unconstitutional deprivation of “fundamental rights and liberty interests.”[191] The discontinuation of LST represents the deprivation of a fundamental right—the right to life----and due process must be satisfied.[192] Accordingly, Section 166.046’s procedural guidelines must require reasonable notice, allow patients’ a meaningful opportunity to be heard, contain ascertainable standards, and require neutral decision makers.[193] Moreover, these guidelines should provide interested parties with the opportunity to participate in the committee review and with the promised ability to present evidence, expert medical testimony, and conduct cross-examination of all witnesses testifying in support of the discontinuation of the LST.[194]
Accordingly, this Author recommends the extension of the forty-eight-hour notice window, implementation of objective standards to guide committee review considerations in determining what is “medically inappropriate,” and implementation of specific committee-member requirements.
A. Extension of the 48-Hour Window.
Extension of the forty-eight-hour window currently required by Section 166.046’s procedural guidelines to a fourteen-day window prevents potential due process violations by providing reasonable notice and a meaningful opportunity to be heard.
Reasonable notice depends on the nature of the case.[195] A case where the discontinuation of LST is determined through an analysis of “medical inappropriateness” presents a question of reasonable medical judgment.[196] The question of medical inappropriateness must require reasonable notice to the parents such that they can present their own evidence that contradicts a physician’s reasonable medical judgment.[197] In other words, the patient should be afforded the opportunity to find a second opinion, in the form of expert medical testimony, to counter the physician opinion urging discontinuation of LST.[198]
A meaningful opportunity to be heard exists when there is sufficient reasonable notice for interested parties to have time to provide the factfinder with evidence in support of their own interests.[199] This extended window provides reasonable time in which parents could find and retain a medical expert who can advocate for the parents’ interests. A medical expert can provide reasonable medical judgment that may refute the attending physician’s recommendation for discontinuation of LST.[200]
The suggested amendment from forty-eight hours to fourteen days will likely be upheld as constitutional because even the shorter, ten-day transfer window has not been questioned for violation of due process.
B. Proposed Objective Standards for Section 166.046
This Note suggests that Section 166.046 should include a factor-based, objective evidentiary standard that considers factors tied to both the parents’ subjective desires and the medical evidence provided by all parties and provide an objective definition of “medically inappropriate.” Objective standardization of factors considered during committee review and standardization of the term “medically inappropriate” will allow all parties a meaningful opportunity to be heard as required under due process.
While Section 166.046 explicitly requires either an ethical or medical committee to review medical inappropriateness, the statute fails to provide objective standards considered by the review committee in coming to its final decision. Beyond establishing this requirement, it only vaguely outlines the details of an ethical or medical committee’s review process when deciding these disputes.[201] Currently, TADA places the burden of deciding medical inappropriateness in the hands of ethical or medical committees but has provided virtually no clarification as to the details of those ethical or medical committees.[202]
Section 166.046 should outline a non-exhaustive list of factors to be considered by the review committee. Such factors should consider the subjective wishes of the parents, the reasons for these wishes, the patient’s quality of life and degree of pain, the treatment already provided, the benefits of any remaining treatment options, and other similar factors.[203] Such implementation provides parents reasonable notice to review standards and provides the review committee with objective factors to consider, analyze, and weigh in their final determination.
Further, the objectivity standard should apply the “best interest” standard’s limited, objective approach, whereby the burden of proof is clear and convincing evidence.[204] When a terminally ill child is legally without parents, discontinuation of LST is only appropriate when evidence objectively demonstrates that the discontinuation of LST is in the “best interests” of the child.[205] This means that in a case where a medical determination is the final conclusion, medical objectivity should be considered the most trustworthy evidence.[206] As a result, the evidentiary standard for determining “medical inappropriateness” would require analyzing whether the evidence provides that continuation of LST would lead to “the burden of a prolonged life from the experience of pain and suffering” that would “markedly outweigh[ ] [life’s] satisfactions.”[207] Thus, continuation of LST would be “medically inappropriate” if continuation of life is “markedly outweighed” by the patient’s pain and suffering.[208] The provision of such a definition provides all parties with reasonable notice and a meaningful opportunity to be heard and allows parties to discern exactly what needs to be proven by clear and convincing evidence.
Section 166.046’s current procedural guidelines must be amended in a manner that extends the forty-eight-hour notice window and implements objective, committee-review evidentiary standards. Without these changes, it fails to meet due process sufficiency requirements, and, as such, ceases to be effective.
C. Committee Standards
Finally, like the evidentiary standards recommended, there should be standards implemented as to committee-member composition. Because one party in a Section 166.046 dispute is typically a lay person and the other is a physician, the committee should be half lay people and half healthcare staff. Through this composition, the jury becomes a jury of peers for both parties, and the decision considers medical reasoning plus holistic, human reasoning.
VIII. Conclusion
We live in an age of medical advancements intended to preserve or prolong life through science and medical intervention; however, there are times when prolongation of life should not be acceptable—for example, when a pediatric patient’s pain and suffering would be markedly outweighed by any subjective parents’ desire for their child to live. From a public policy standpoint, Section 166.046 is critical in ensuring that the prolongation of life through continuation of LST does not exist in those situations.
Changes to current procedural guidelines must be implemented for its effectiveness not to be barred by constitutional due process requirements; thus, the extension of the forty-eight-hour notice window and the implementation of objective standards in its procedural guidelines are key to protecting the ethical intent of the act and to correcting the current procedural unconstitutionality.
Karina Sanchez
Megan McDonnell Busenbark, 25 Changes in 25 Years, Child.'s Hosp. Today, Winter 2017, at 18, 19–23, https://www.nxtbook.com/nxtbooks/cha/cht_2017winter/index.php#/p/18 [https://perma.cc/T573-RTSE].
The modern surgical procedures, supportive treatments, medical tools, and evidence-based practice in action today have transformed pediatric care in the last two decades. See Alan Meisel & Bruce Jennings, Ethics, End-of-Life Care, and the Law: Overview, in Living with Grief: Ethical Dilemmas at the End of Life 63, 63 (Kenneth J. Doka et al. eds., 2005) (“Most of the cases and dilemmas that have shaped the law on end-of-life care have involved patients whose lives could be prolonged by new medical treatments and technologies, but whose health, functioning, quality of life, and even conscious awareness itself could not be restored.”); see also Busenbark supra note 3 (showcasing twenty-five advancements in pediatric care in the last twenty-five years).
See Andrew H. Malcolm, Extending Life or Prolonging Death?, N.Y. Times, Mar. 23, 1986, at 24, https://www.nytimes.com/1986/03/23/weekinreview/extending-life-or-prolonging-death.html [https://perma.cc/PDY6-GAWG] (“When should the technology be used to prolong life and when does it merely prolong dying? One person’s salvation is another’s living hell.”); U.S. Const. amend. XIV, § 1 (“[N]or shall any State deprive any person of life, liberty, or property, without due process of law . . . .”).
See Brian Mastroianni, From Vaccines and Gene Editing to Malaria Treatment: The Important Medical Innovations of 2021, Healthline (Dec. 27, 2021), https://www.healthline.com/health-news/from-vaccines-and-gene-editing-to-malaria-treatments-the-important-medical-innovations-of-2021 [https://perma.cc/92KE-BXK5] (“We’ve got drugs that prolong lives, prevent heart failure hospitalizations, the ability to really change the quality of life for our heart failure patients. It’s a whole new world,” he said. “Some of my colleagues have changed from calling it ‘heart failure’ to ‘heart success.’” (quoting Dr. Donald Llyod-Jones, President of the American Heart Association)).
Health & Safety § 166.046.
Id. § 166.031(2).
See id. §§ 166.034–.035, .046.
Id. § 166.002(3).
Id. §§ 166.002(10), .031(1), .032(a), .032(d), .033. A patient’s adult spouse, parents, or legal guardian “may execute a directive on behalf of a qualified patient who is younger than 18 years of age” under TADA. Id. § 166.035.
Id. § 166.002(10).
See id. §§ 166.002, .046; see also Martin L. Smith, Medical Inappropriateness Review: Appropriately Performed by a Medical Committee, 18 Health Matrix: J.L.—Med. 237, 241 (2008) (explaining that “TADA does not define ‘medical appropriateness,’ or ‘medical inappropriateness’”).
Health & Safety §§ 166.002, .046; see also Smith, supra note 13, at 237 (explaining that “TADA neither specifies a preference for the type of review committee, nor the membership composition of either committee”).
A colloquial name given to the EMS phone at the Emergency Department’s nurse triage station where ambulances call in to report an incoming critical case. See, e.g., Carmella Mataloni, Wayne Memorial Hospital Enhances Emergency Services, WNEP (Feb. 16, 2017, 4:53 PM), https://www.wnep.com/article/news/local/wayne-county/wayne-memorial-hospital-enhances-emergency-services/523-96b110b9-4dc7-4f8c-8970-811c4697ace1 [https://perma.cc/PYL7-XGWB].
See Health & Safety § 166.046; Peter A. Clark, Medical Futility: Legal and Ethical Analysis, 9 AMA J. of Ethics 375, 376 (2007) (quoting Robert L. Fine & Thomas W. Mayo, Resolution of Futility by Due Process: Early Experience with the Texas Advance Directives Act, 138 Annals of Internal Med. 743, 744 (2003)) (available at https://journalofethics.ama-assn.org/article/medical-futility-legal-and-ethical-analysis/2007-05) [https://perma.cc/2VP7-5QJU]; see also Robert L. Fine, Medical Futility and the Texas Advance Directives Act of 1999, 13 Baylor U. Med. Ctr. Procs. 144, 145–46 (2000).
. Health & Safety § 166.046(a).
See supra text accompanying note 13; discussion infra Section III.A.
Health & Safety § 166.046(e); see Fine, supra note 16, at 144–45.
See Fine, supra note 16, at 145.
In re Quinlan, 355 A.2d 647, 662–64, 668–69 (N.J. Sup. Ct. 1976); Karen Teel, The Physician’s Dilemma: A Doctor’s View: What the Law Should Be, 27 Baylor L. Rev. 6, 8–9 (1975).
Quinlan, 355 A.2d at 662–63, 669; see Elizabeth Gmyrek England, Note, The Debate on Physician-Assisted Suicide Reaches the Federal Courts. A Discussion of the Decisions of the District and Circuit Courts in Compassion in Dying v. Washington State, 16 Pace L. Rev. 359, 378 (1996).
See Fine, supra note 16, at 145.
Id.
Id.
Id.; Robert H. Shmerling, First, Do No Harm, Harv. Health Publ’g: Harv. Health Blog (Jun. 22, 2020), https://www.health.harvard.edu/blog/first-do-no-harm-201510138421 [https://perma.cc/X2AL-E9RX].
Fine, supra note 16, at 145 (quoting Selections from the Hippocratic Corpus: "The Art", in Ethics in Medicine: Historical Perspectives and Contemporary Concerns, 5, 6 (Stanley Joel Reiser, et al. eds., MIT Press 1977)).
Id.
Id.
Id.
Id.
Id.
Id.
Id. (emphasis added).
Id.
Id.
Id.; see Clark, supra note 16, at 375, 381.
Nora O’Callaghan, Dying for Due Process: The Unconstitutional Medical Futility Provision of the Texas Advance Directives Act, 60 Baylor L. Rev. 527, 536 (2008). While the report provided procedural suggestions for futility determinations, no definition was given. See id.; Tex. Health & Safety Code § 166.046.
Fine, supra note 16, at 145.
Id.
Id.
Sen. Rsch. Ctr., Bill Analysis, Tex. S.B. 1260, 76th Leg., Reg. Sess. (1999); Jamie Stengle, Spotlight on Texas’ ‘10-Day Rule’ in Life Support Cases, Austin Am.-Statesman (Nov. 13, 2019, 5:00 AM), https://www.statesman.com/story/news/2019/11/13/spotlight-on-texas-10-day-rule-in-life-support-cases/2305176007/ [https://perma.cc/5NBD-5983]. Further, Stakeholder groups like the Texas and National Right to Life, Texas Alliance for Life, the Texas Conference of Catholic Health Care Facilities, the Texas Medical Association, the Texas Hospital Association, and the Texas and New Mexico Hospice Organization were involved. See Relating to Advance Directives for Medical Treatment; Providing Administrative Penalties: Hearing on H.B. 3527 Before the H. Comm. on Pub. Health, 1999 Leg., 76th Sess. (Tex. 1999) (statement of Greg Hooser, Tex. and N.M. Org.).
Thaddeus Pope, Procedural Due Process and Intramural Hospital Dispute Resolution Mechanisms: The Texas Advance Directives Act, 10 St. Louis U. J. of Health L. & Pol’y 93, 112 (2016).
See Tex. Health & Safety Code § 166.046.
See Thomas William Mayo, The Baby Doe Rules and Texas’s “Futility Law” in the NICU, 25 Ga. St. U. L. Rev. 1003, 1004 & n.6 (2009).
See Health & Safety § 166.046.
See Clark, supra note 16, at 376; Fine, supra note 16, at 145–46.
Health & Safety § 166.046(a), (e).
Id.
Id. § 166.046(b)(1)–(2).
Id. §§ 166.046(b)(3), .052(a), .053(a).
Id. § 166.053(a).
Id. § 166.046(b)(4)(A)–(D).
Id. § 166.046(d).
See id. § 166.002.
Id. § 166.046(a), (e).
Id. § 166.046(e). Before the expiration of the ten days, the patient representative may then pursue judicial methods by filing a request to “the appropriate district or county court” for an extension. Id. § 166.046(e), (g). The court must grant the extension “if the court finds, by a preponderance of the evidence, that there is a reasonable expectation” that an alternate physician or healthcare facility will accept the transfer of care upon extension. Id. § 166.046(g). If the court finds that a reasonable expectation exists, the LST must be continued in the interim up until the transfer or expiration of the extension. Id. § 166.046(e), (g).
Id. § 166.046(e).
Id. § 166.046(d).
Id. § 166.046(e).
Id. § 166.046(g).
Id. § 166.046(e), (g).
Id.
While Section 166.046 currently has procedural requirements that, in part, include notice, just having a process in place for the provision of notice does not mean that due process has been satisfied. Id. § 166.046 (b)(1)–(2); T.L. v. Cook Child. Med. Ctr., 607 S.W.3d 9, 76, 83 (Tex. App.—Fort Worth 2020, pet. denied) (noting that the applicable standard is the Mullane standard, not the Mathews v. Eldridge balancing test; and then quoting Mullane v. Cent. Hanover Bank & Tr., 339 U.S. 306, 313 (1950) (identifying that the Due Process clause “require[s] that deprivation of life, liberty or property by adjudication be preceded by notice and opportunity for hearing appropriate to the nature of the case”)).
Health & Safety § 166.046(b)(1)–(2).
T.L., 607 S.W.3d at 83.
Id. at 85.
Id. at 83.
Id. at 84; see also Health & Safety §§ 166.002(9), .002(13), .040(a).
T.L., 607 S.W.3d at 83–84.
And even if they were, their role has not been a medical one throughout the patient’s medical care.
T.L., 607 S.W.3d at 83–84.
Id. at 84 (quoting Sloan v. Molandes, 32 S.W.3d 745, 747–48 (Tex. App.—Beaumont 2000, no pet.)). As Section 166.046 is silent on this matter, we additionally refer to the malpractice context in cases of terminal or irreversible medical conditions. Health & Safety § 166.046. In these cases, expert medical testimony is necessary and required. See Fenley v. Hospice in the Pines, 4 S.W.3d 476, 481–85 (Tex. App.—Beaumont 1999, pet. denied) (reversing summary judgment based on expert testimony demonstrating misdiagnosis of the terminal and irreversible prognosis).
T.L., 607 S.W.3d at 84.
Goldberg v. Kelly, 397 U.S. 254, 257–62, 264–71 (1970); see U.S. Const. amend. XIV, § 1.
Health & Safety § 166.046(a).
Id. § 166.002(6).
Id. § 161.031(a).
Id. § 161.0315.
“(1) a hospital; (2) a medical organization; (3) a university medical school or health science center; (4) a health maintenance organization . . . ; (5) an extended care facility; (6) a hospital district; and (7) a hospital authority.” Id. §§ 161.031(a), .0315(a).
Id. § 166.046(a).
Id. While Section 166.046 is an extrajudicial process, patients have brought judicial claims concerning Section 166.046 and committee decisions to the courts. T.L. v. Cook Child. Med. Ctr., 607 S.W.3d 9, 24 n.8, 32 (Tex. App.—Fort Worth 2020, pet. denied).
T.L., 607 S.W.3d at 28–30.
Id. at 29.
Id. at 29–30.
See Health & Safety § 166.046(a) (“[T]he physician’s refusal shall be reviewed by an ethics or medical committee.”); Ronald D. Rotunda & John E. Nowak, Treatise on Constitutional Law: Substance and Procedure 100 (3rd ed. 1999) (“[T]here is always the general requirement that the government process be fair and impartial. Therefore, there must be some type of neutral and detached decision-maker . . . .”).
Rotunda & Nowak, supra note 86, at 100.
See, e.g., T.L., 607 S.W.3d at 29–30 (noting that nineteen of the twenty-two committee members were the attending physician’s co-workers).
Id. at 59 n.29.
In re Murchison, 349 U.S. 133, 136 (1955).
O’Callaghan, supra note 38, at 600.
T.L., 607 S.W.3d at 90.
Health, Data USA, https://datausa.io/profile/cip/health?redirect=true [https://perma.cc/87JM-RKNT] (last visited Dec. 15, 2022).
. Tex. Health & Safety Code § 166.046(a).
Id. §§ 166.046(e), .052(a).
See generally Health & Safety.
Please note that the Texas Administrative Code acknowledges “the right of the patient or the patient’s designated representative to participate in the consideration of ethical issues that arise in the care of the patient.” 25 Tex. Admin. Code § 133.42(a)(1)(F). Without providing notice of the objective considerations a review committee should consider in coming to its determination regarding the continuation of LST—an ethical issue that trumps all others—this right is violated, and notice is insufficient. This is a separate argument, but worth noting.
See generally Health & Safety.
Mullane v. Cent. Hanover Bank & Tr., 339 U.S. 306, 314–15; Pope, supra note 43, at 142.
See Health & Safety § 166.046(e); see also T.L. v. Cook’s Child. Med. Ctr., 607 S.W.3d 9, 91–92 (Tex. App—Fort Worth 2020, pet. denied).
T.L., 607 S.W.3d at 85 (asserting that insufficient notice and inability to properly advocate exists when there is no objective information provided).
Robert D. Truog, Medical Futility, 25 Ga. St. U. L. Rev. 985, 985 (2012).
See T.L., 607 S.W.3d at 28–29.
See infra Sections V.A–B.
See infra Sections V.A–B.
Truog, supra note 102, at 985.
Id.
Id.
Id.
Id. at 985–86.
Id.
Ralph D. Feign & Laurence B. McCullough, The Tragedy of Sun Hudson, Chron (Mar. 27, 2005), https://www.chron.com/opinion/outlook/article/The-tragedy-of-Sun-Hudson-1947366.php [https://perma.cc/ZDG6-MCQX].
Id.
Id.
Id.
Id.
Id.
See Truog, supra note 102, at 985.
Feign & McCullough, supra note 112.
Truog, supra note 102, at 985–86.
Feign & McCullough, supra note 112.
Truog, supra note 102, at 986.
See Clark, supra note 16, at 377.
T.L. v. Cook Child. Med. Ctr., 607 S.W.3d 9, 26 (Tex. App.—Fort Worth 2020, pet. denied); About Cook Children’s, CookChild.'s, https://www.cookchildrens.org/about/ [https://perma.cc/8Z3L-XPGR] (last visited Jan. 27, 2022).
Michael Williams, Fort Worth Court Will Determine Who Decides Severely Ill Toddler’s Medical Care. Mom or Her Doctors?, Dall. Morning News (Sept. 23, 2021, 4:16 PM), https://www.dallasnews.com/news/public-health/2021/09/23/fort-worth-court-will-determine-who-decides-severely-ill-toddlers-medical-care-mom-or-her-doctors/ [https://perma.cc/LAP6-9QXD]; T.L., 607 S.W.3d at 26.
Ebstein Anomaly, Mayo Clinic, https://www.mayoclinic.org/diseases-conditions/ebsteins-anomaly/symptoms-causes/syc-20352127 [https://perma.cc/868T-8HQW] (last visited Jan. 26, 202).
T.L., 607 S.W.3d at 26.
Id. at 27.
Id.
Id.
Id.
Id.
Eventually, Tinslee had a nasogastric tube in her nose, multiple IVs, and a tube connecting her to the ventilator. All these tubes were necessary for her to receive oxygenation, medication, hydration, and nutrition. Id.
Id. at 27–28.
Id. at 27.
Id. at 27–28.
Id. at 28.
Id.
Id.
Id.
Id.
Id. (“[Nurses] eventually opt[ed] to take shifts that would not involve caring for [Tinslee] to avoid [the] emotional distress of watching her suffer.”).
Id.
Id.; Charles Scudder, 6 Things to Know About Tinslee Lewis, the Fort Worth Infant on Life Support at Cook Children’s, Dall. Morning News (Jan. 4, 2020, 6:30 AM), https://www.dallasnews.com/news/courts/2020/01/04/6-things-to-know-about-tisnlee-lewis-the-fort-worth-infant-on-life-support-at-cook-childrens/ [https://perma.cc/KHW2-8M73].
T.L., 607 S.W.3d at 28.
Id. at 28.
Id. at 28–29.
Id. at 29.
Id.
Id.
Id.
Id.
Id.
Id.
Id.
Id.
Id. at 29–30.
Of the twenty-five total committee members, twenty-two showed up. Nineteen of these twenty-two were active Cook Children’s Medical Center employees. Id.
Id. at 30.
Id.
Id.
Id.
Id.
See id. at 31.
Id. at 30.
Id.
Id.
Id. at 31.
Scudder, supra note 144.
T.L., 607 S.W.3d at 32.
Id.
Id.
Tinslee’s mother “alleg[ed] that [(1) Cook Children’s] decision to discontinue [LST] interfered with her . . . right as a parent to make treatment decisions and . . . violated [Tinslee’s] right to life . . . without providing sufficient procedural-due-process protection;” and (2) TADA § 166.046 is unconstitutional “due to a lack of substantive and procedural due process.” Id. As a result, a hearing was set for November 22, 2019, and Cook Children’s was ordered to continue providing LST until November 23, 2019. See id; Sarah McConnell, Hearing for Tinslee Lewis’ Life Support Case Extended to December, Texan (Nov. 20, 2019), https://thetexan.news/hearing-on-tinslee-lewis-life-support-case-scheduled-for-friday/ [https://perma.cc/5VSQ-9QY6].
T.L., 607 S.W.3d at 32.
See id. at 31–33.
Id. at 32.
Id.
Id. at 34–35.
Id. at 34.
Id. at 94—95.
Id. at 23.
Id. at 83, 89.
Id. at 94.
See Cook Child. Med. Ctr. v. T.L., 141 S. Ct. 1069 (2021).
See T.L., 607 S.W.3d at 94.
Feign & McCullough, supra note 112.
Id.
See supra Section V.B.
T.L., 607 S.W.3d at 28.
Scudder & Steele, supra note 1.
Cook Children’s Medical Center’s Brief in Response to Plaintiff’s Request for Injunctive Relief at 3, T.L., 607 S.W.3d 9 (No. 323-112330-19).
See supra Sections V.A–B.
T.L., 607 S.W.3d at 36–37 (quoting Washington v. Glucksberg, 521 U.S. 702, 720 (1997)); U.S. Const. amend. XIV, § 1.
T.L., 607 S.W.3d at 80 (citing Parham v. J.R., 442 U.S. 584, 600 (1979)).
See id. at 92–93.
See Goldberg v. Kelly, 397 U.S. 254, 267–69 (1970); U.S. Const. amend. XIV.
See Mullane v. Cent. Hanover Bank & Tr., 339 U.S. 306, 313 (1950).
T.L., 607 S.W.3d at 84.
Id. at 86.
Id.; cf. Sloan v. Molandes, 32 S.W.3d 745, 747–48 (Tex. App.—Beaumont 2000, no pet.) (secondary medical expert testimony is used to prove doctor violated the relative standard of care).
U.S. Const. amend. XIV; Mullane, 339 U.S. at 313–14.
Goldberg v. Kelly, 397 U.S. 254, 264–71 (1970).
See Tex. Health & Safety Code § 166.046.
See id. § 166.046(a), (e).
See In re Christopher I., 131 Cal. Rptr. 2d 122, 134–35 (Cal. Ct. App. 2003) (outlining the factors to be considered for discontinuation of LST) (“[A] court making the decision of whether to withhold or withdraw life-sustaining medical treatment from a dependent child should consider . . . : (1) the child’s present levels of physical, sensory, emotional, and cognitive functioning; (2) the quality of life, life expectancy, and prognosis for recovery with and without treatment, including the futility of continued treatment; (3) the various treatment options, and the risks, side effects, and benefits of each; (4) the nature and degree of physical pain or suffering resulting from the medical condition; (5) whether the medical treatment being provided is causing or may cause pain, suffering, or serious complications; (6) the pain or suffering to the child if the medical treatment is withdrawn; (7) whether any particular treatment would be proportionate or disproportionate in terms of the benefits to be gained by the child versus the burdens caused to the child; (8) the likelihood that pain or suffering resulting from withholding or withdrawal of treatment could be avoided or minimized; (9) the degree of humiliation, dependence, and loss of dignity resulting from the condition and treatment; (10) the opinions of the family, the reasons behind those opinions, and the reasons why the family either has no opinion or cannot agree on a course of treatment; (11) the motivations of the family in advocating a particular course of treatment; and (12) the child’s preference, if it can be ascertained, for treatment.”).
Id.
See Cruzan v. Dir., Mo. Dep’t of Health, 497 U.S. 261, 272–73 (1990) (discussing the approach adopted by the New Jersey Supreme Court in In re Conroy, 486 A.2d 1209 (N.J. 1985)).
See Cruzan, 497 U.S. at 273 (discussing the approach adopted by the New Jersey Supreme Court in Conroy, 486 A.2d 1209).
Id.
Id.